Wayne County Speech-Language Guidelines

Wayne RESA, in collaboration with local district representatives, has put together information on the following topics regarding speech and language services in Wayne County. Included in this page's accordions below are guidance information, forms, and links to frequently asked questions (FAQ).
Resources
These resources were compiled from a variety of professional organizations and educational agencies:
- American Speech-Language-Hearing Association (ASHA)(External Website, opens in new window)
- Guidelines for Speech & Language Evaluation, Eligibility and Service Delivery in Schools (MSHA, 2025)(PDF, opens in new window)
- Kent County ISD Speech and Language Evaluation, Eligibility and Service Guidelines (2021)(PDF, opens in new window)
- Michigan Administrative Rules for Special Education (MARSE) With Related IDEA Federal Regulations(PDF, opens in new window)
- Michigan Speech-Language Guidelines (2006)(PDF, opens in new window)
Caseload / Workload and Service Delivery
Overview
Per MARSE R 340.1745, the following provisions are specific requirements for school-based speech and language services:
- Services must be based on student needs as determined by the IEP team after reviewing a diagnostic report provided by an authorized speech and language provider.
- Caseload size is determined by the provider in cooperation with the district director of special education and building principals. Decisions must consider disability severity and the extent of service required, allowing dedicated time for:
- (i) Diagnostics
- (ii) Report writing
- (iii) Consulting with parent/guardians and teachers
- (iv) Individualized education program (IEP) team meetings
- (v) Travel
- Individual caseloads shall not exceed 60 different persons and must be adjusted based on the factors above. Students currently being evaluated are counted as part of the caseload.
Workload vs. Caseload
Workload refers to all activities performed by school-based SLPs, while Caseload is just the number of students served. A workload analysis approach ensures that professionals have sufficient time to meet individual student needs under IDEA. This includes mandated IEP activities as well as MTSS/RtI participation and staff training.
- ASHA Practice Portal: Caseload and Workload(External Website, opens in new window)
- ASHA Implementation Guide: Workload Analysis Approach(External Website, opens in new window)
Service Delivery
SLPs are responsible for selecting evidence-based service delivery models that are flexible, outcome-oriented, and curriculum-based. IDEA mandates that services occur in the Least Restrictive Environment (LRE), which may include the classroom or alternate settings. Common formats include:
- Traditional Weekly, Receding, or Cyclical Schedules
- Block, Blast, or Burst Scheduling
- Group Size Considerations
Least Restrictive Environment (LRE)
To the maximum extent possible, students must be educated with non-disabled peers. Providing speech and language services within the classroom facilitates the generalization of skills, promotes teacher-SLP collaboration, and ensures treatment is directly relevant to the general education curriculum.
Additional Resources
Evaluation / Eligibility Overview
Eligibility
Speech-Language Impairment (SLI), as defined in MARSE 340.1710(PDF, opens in new window), can be a primary or secondary eligibility. To qualify, an adverse educational impact is required in one or more areas: language, articulation, fluency, and/or voice. Considerations must be given to academic, vocational, and social-emotional factors.
Academic Impact
Students may have difficulty with:
- Reading, math, and language arts (grades-based impact)
- Language-based activities and phonological awareness
- Comprehending information from text or oral presentations
- Decoding, sound/letter correspondence, and encoding
- Reading fluency and solving math word problems
- Putting thoughts into writing or relating narratives in sequence
- Being understood during classroom assessments
Social-Emotional Impact
Students may have difficulty with:
- Being understood by others or experiencing teasing from peers
- Maintaining and terminating verbal interactions
- Making and maintaining friendships
- Feelings of embarrassment or frustration
- Expressing emotions during social situations or conflict resolution
*Note: If a student does not experience a negative perception of their own speech, they may not benefit from treatment at that time.
Vocational Impact
Job-related skills impacted by SLI include:
- Understanding and following oral directions
- Inappropriate responses to coworkers or supervisors
- Inability to ask/answer questions in a coherent manner
- Difficulty being understood when speaking
Standard Evaluation Process
Prior to evaluation, it is highly recommended that the district’s Multi-Tiered System of Support (MTSS) be reviewed. Standard practice in Michigan often involves qualifying students with scores 1 and 1/3 standard deviations below the mean (Standard Score of 80 or below). However, SLPs should select tests with high sensitivity and specificity (>80%) and consult specific test manuals for cut-off recommendations. A single test score should not be the sole determinant for eligibility.
Additional Resources
Standard Speech and Language Evaluation Process Components
Evaluation Tools and Forms
The following resources and forms are provided to assist Speech-Language Pathologists in conducting comprehensive evaluations and screenings.
- Bell Curve Handout(PDF, opens in new window)
- Bilinguistics Free Assessment Materials(External Website, opens in new window)
- Case History Form(PDF, opens in new window)
- Checklist for Reviewing Norm-Referenced Tests(Google Doc, opens in new window)
- Communication Matrix(External Website, opens in new window)
- Dynamic Assessment Goals Grid-3 (DAGG-2)(PDF via Google Drive, opens in new window)
- Elementary Informal Language Sample Checklist(PDF, opens in new window)
- FAQ: Speech Sound Disorders Input Forms(Google Doc, opens in new window)
- FAQ: Language Input Forms(Google Doc, opens in new window)
- FAQ: Fluency Input Forms(Google Doc, opens in new window)
- Fluency Speech Sample Worksheet(PDF, opens in new window)
- MARSE ASD Eligibility Observation Form(PDF, opens in new window)
- MARSE ASD Eligibility Observation Form (Preschool)(PDF, opens in new window)
- Oral Peripheral Mechanism Exam(PDF, opens in new window)
- Screening Report Form(PDF, opens in new window)
- School-age Language Assessment Measures (SLAM)(External Website, opens in new window)
- SETT Framework Template(Google Doc, opens in new window)
- SETT Framework Resources (Joy Zabala)(External Website, opens in new window)
- The Rainbow Passage(PDF, opens in new window)
- Voice Input Forms(Google Doc, opens in new window)
Speech Sound Disorders: Articulation and Phonology
 Overview
Overview
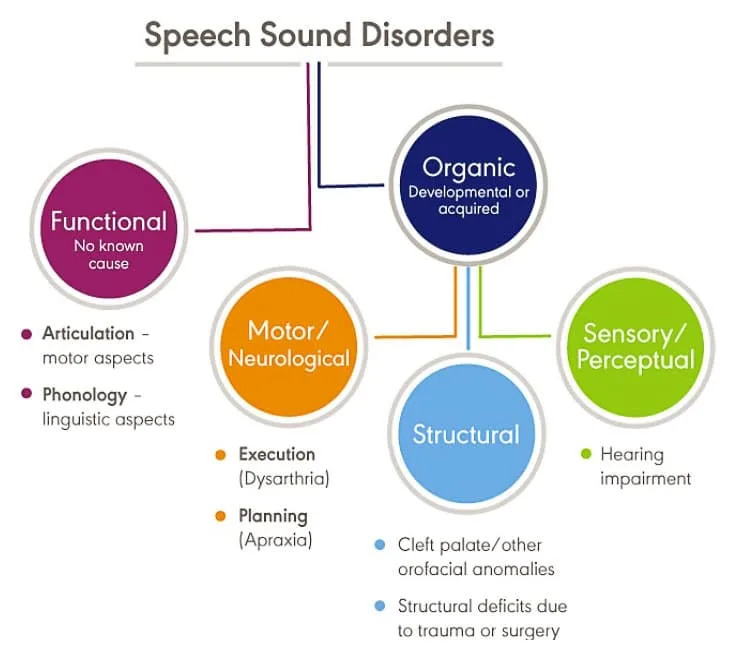
This resource supports school teams in identifying and serving students (ages 0-26) with speech sound disorders. This "umbrella term" encompasses difficulties with perception, motor production, or phonological representation of speech sounds. Our goal is to ensure consistency in services throughout Wayne County by outlining the evaluation process, service delivery, and exit criteria.
When concerns arise, consultation with an SLP is the first step. If articulation errors can be resolved without direct intervention, the SLP may suggest classroom strategies. For students needing more support, the district's MTSS process should be utilized. If data shows a student is not making appropriate progress despite these interventions, the formal special education evaluation process may be initiated.
Evaluation & Eligibility
In addition to standard evaluation procedures, SLPs should focus on specific assessment areas based on the student's age:
- 0-3 Years: Intelligibility, syllable shapes, and vowel sound production.
- 3-5 Years: Intelligibility, phonological processes, and stimulability.
- 6-9 Years: Speech sound production norms and stimulability. Social and academic impacts gain higher importance here.
- 9+ Years: Stimulability and social/academic/vocational considerations are the primary focus.
Test scores and standard deviations must not be the sole criteria for eligibility. The disability must adversely affect educational performance (social, academic, or functional).
- Intelligibility Norm Chart(External Website, opens in new window)
- Articulation Norms: Crowe and McLeod (2020)(PDF, opens in new window) — A conservative perspective on consonant acquisition.
- Articulation Norms: Goldman Fristoe (2015)(PDF, opens in new window) — A more liberal perspective on acquisition.
- Speech Sound Production Severity Rating Scale(PDF, opens in new window)
- Phonological Processes Chart(PDF, opens in new window)
- Oral Peripheral Mechanism Exam Form(PDF, opens in new window)
Service Delivery
Intervention programs should provide daily opportunities for practice within the classroom or home setting using curriculum-relevant materials. Frequency should align with severity and individual student needs. For assistance in determining the appropriate service level, refer to the matrix below:
Exit Criteria
Research suggests that students dismissed at 75-85% accuracy in conversational speech often continue to fully self-correct. Per MSHA and ASHA guidelines, services should be discontinued if minimal progress is documented over one to two consecutive years despite varied approaches. This ensures the student remains in the Least Restrictive Environment (LRE) when specialized services no longer provide a measurable benefit.
Input Forms: Student, Parent, and Teacher
- Speech Sounds: Student Input Form(PDF, opens in new window)
- Speech Sounds: Parent Input Form(PDF, opens in new window)
- Teacher Input: Grades K-2(PDF, opens in new window)
- Teacher Input: Grades 3-5(PDF, opens in new window)
- Teacher Input: Middle School(PDF, opens in new window)
- Teacher Input: High School(PDF, opens in new window)
Additional Resources
Language
Overview
When a teacher or parent has concerns about a student’s language development, the student should be brought to the school’s student success or child study team. General education interventions (RtI, observations, data gathering) should be implemented unless Child Find is triggered. If interventions do not indicate progress, the team must proceed with a formal evaluation.
Language impairment is the inadequate or inappropriate acquisition, comprehension, or expression of language. It can affect spoken language, written language, and/or the use of an AAC system. These impairments are generally categorized into:
- Form: Phonology, Morphology, Syntax
- Content: Semantics
- Use: Pragmatics
While MARSE utilizes the term "Speech and Language Impairment" (SLI), SLPs should also be familiar with Developmental Language Disorder (DLD). This refers to language difficulties not associated with a known biomedical condition, which may coincide with challenges in motor coordination, attention, or executive function.
Evaluation and Eligibility
To qualify under MARSE guidelines, inadequate language functioning must be demonstrated through a language sample and at least two standardized assessments or subtests. A comprehensive assessment includes:
- Standardized and Dynamic Assessments
- Discourse and Narrative Sampling
- Systematic Observation and Contextual Analysis
- Parent/Teacher/Student Report Measures
- Consideration of Language Diversity and Severity Ratings
The IEP team must determine how language deficits adversely impact the student’s education compared to same-age peers.
- Child Find Procedural Guide(PDF, opens in new window)
- MARSE Guidelines (Eligibility Criteria)(PDF, opens in new window)
- Language Severity Rating Scale(Google Drive Link, opens in new window)
Language Impairments Reference
Spoken Language Impairments
| Domain | Listening (Receptive) | Speaking (Expressive) |
|---|---|---|
| Phonology | Identifying and distinguishing phonemes (phonological awareness) | Appropriate use of phonological patterns |
| Morphology | Understanding morphemes (word parts) | Using morphemes correctly |
| Syntax | Understanding sentence structure elements | Using correct sentence structure |
| Semantics | Listening vocabulary | Speaking vocabulary |
| Pragmatics | Understanding social aspects of spoken language | Social use of language and cohesive messages |
Written Language Impairments
| Domain | Reading | Writing |
|---|---|---|
| Phonology | Letter-sound associations (phonics) | Accurate spelling of words |
| Morphology | Understanding grammar while reading | Appropriate use of grammar in writing |
| Syntax | Understanding sentence structure while reading | Using correct sentence structure in writing |
| Semantics | Reading vocabulary | Writing vocabulary |
| Pragmatics | Understanding point-of-view and audience needs | Conveying point-of-view and intended messages |
Input Forms: Student and Teacher
Fluency
Overview
 When concerns regarding a student’s speech fluency arise, teachers or parents should consult with an SLP to determine if further assessment is necessary. If the team determines that disfluency may be resolved through indirect support, the SLP provides strategies for the parent, student, and teacher. If disfluencies persist despite these strategies, a formal speech-language evaluation may be initiated.
When concerns regarding a student’s speech fluency arise, teachers or parents should consult with an SLP to determine if further assessment is necessary. If the team determines that disfluency may be resolved through indirect support, the SLP provides strategies for the parent, student, and teacher. If disfluencies persist despite these strategies, a formal speech-language evaluation may be initiated.
Definitions
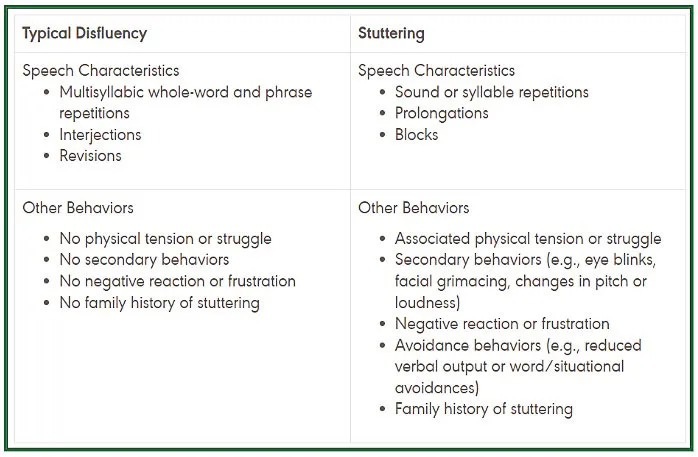
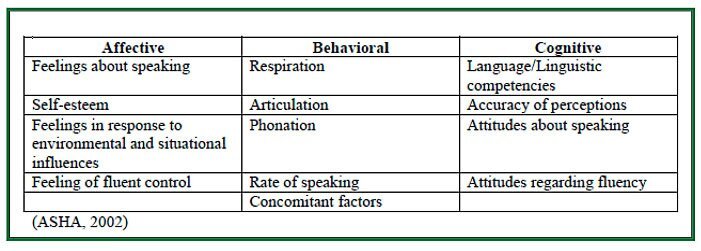
Stuttering: An interruption in the flow of speaking characterized by repetitions (sounds, syllables, words, phrases), prolongations, blocks, interjections, and revisions. These may be accompanied by physical tension, negative reactions, secondary behaviors, and avoidance of speaking situations.
Cluttering: A disorder of speech and language processing resulting in rapid, dysrhythmic, sporadic, and frequently unintelligible speech. While accelerated speech is common, an impairment in language formulation is almost always present.
Evaluation & Eligibility
 Eligibility is determined by whether the student experiences an adverse educational effect, which includes academic, social, behavioral, and emotional success. If a child limits class participation, has reduced social interaction, or expresses fear or concern about their speech, intervention is indicated.
Eligibility is determined by whether the student experiences an adverse educational effect, which includes academic, social, behavioral, and emotional success. If a child limits class participation, has reduced social interaction, or expresses fear or concern about their speech, intervention is indicated.
The SLP also considers specific risk factors (such as family history or duration of disfluency) to determine whether to monitor the student informally or expedite formal treatment.
Service Delivery
The IEP Team selects service delivery options designed to increase the student's participation and progress in the general education curriculum. Options should be reviewed and adjusted as the student’s needs change.
- ASHA: School-Based Service Delivery(External Website, opens in new window)
- Severity/Intervention Matrix for Speech and Language Services(PDF, opens in new window)
Exit Considerations
Benchmarks for success are not based solely on the frequency of stuttering. A student may stutter frequently but have a low functional impact, while another may stutter less but experience high levels of frustration or secondary behaviors. Dismissal is considered when the student has met their communication goals or when services no longer provide a measurable benefit to their educational access.
Input Forms: Student, Parent, and Teacher
- Fluency: Student Input (Grades K-4)(PDF, opens in new window)
- Fluency: Student Input (General)(PDF, opens in new window)
- Fluency: Parent Input Form(PDF, opens in new window)
- Teacher Input: Grades K-2(PDF, opens in new window)
- Teacher Input: Upper Elementary(PDF, opens in new window)
- Teacher Input: Middle School(PDF, opens in new window)
- Teacher Input: High School(PDF, opens in new window)
Severity Rating Scale
Voice
Overview
When a student presents with temporary vocal changes like laryngitis or hyponasality, a brief consultation regarding duration and symptoms (such as a cold or allergies) can often alleviate concern. If the vocal quality does not resolve and appears to adversely affect educational performance, the REED process is initiated. A medical evaluation, typically from an otolaryngologist (ENT), is often requested during this phase to rule out underlying structural or physiological issues.
Definitions
A Voice Disorder occurs when vocal quality, pitch, or loudness is inappropriate for an individual's age, gender, or cultural background. A disorder is present if the individual’s voice does not meet their daily communication needs, even if the deviation is not immediately perceived by others.
Evaluation & Eligibility
The IEP team determines eligibility based on whether the voice disability results in an adverse educational effect (academic, social, or emotional). A comprehensive evaluation includes:
- Vocal Quality: Assessment for breathiness, stridency, or hoarseness, including phonatory efficiency and muscle tension (hypertension/hypotension).
- Pitch: Evaluation of inappropriate pitch levels, pitch breaks, or monotone delivery.
- Loudness: Assessment of excessive loudness or softness.
- Resonance: Investigation of structural abnormalities (e.g., cleft palate, VPI) resulting in hypernasality, hyponasality, or nasal emissions.
- Clinical Measures: Assessment of s/z ratio, maximum phonation time, and breath rate.
Evaluation Resources
- Voice Input Forms: Student, Parent, & Teacher(PDF, opens in new window)
- Oral Peripheral Mechanism Exam Form(PDF, opens in new window)
- CAPE-V Procedures and Clinical Form(PDF, opens in new window)
- Voice Related Quality of Life (V-RQOL) Measure(External Resource, opens in new window)
- Voice Severity Rating Scale Rubric(PDF, opens in new window)
Adverse Impact Examples: Limited classroom participation, difficulty communicating in loud environments (cafeteria/bus), or visible student frustration/embarrassment.
Note: Cultural variations in pitch and volume must be considered. Temporary factors such as allergies, colds, or reflux should not be classified as a permanent voice impairment.
Exit Considerations
A student may be exited from services if the voice disorder is resolved or if the quality no longer has an adverse impact on their educational setting.
Linguistic Diversity and Multilingual Learners
Overview
To help prevent over-representation of racial and/or ethnic groups within specialized instruction, SLPs and school teams should ensure that their structures, policies, and routines account for language diversity and cultural differences. The term language diversity describes the wide variation in communication form, content, and use. For example, variations in vocabulary, morphology, syntax, and phonology may be noted in individuals who communicate in English using regional dialects. Students who are identified as multilingual learners may exhibit communication differences because of language differences, accents, or cultural variations. Students who use a dialect of English other than Standard American English are called bidialectal (e.g., individuals using African American English or a Southern dialect who are also expected to use Standard American English in school).
Evaluation
A student must present a language disorder in both languages to qualify as a person with a speech-language disorder. SLPs should use a variety of assessments and modifications to account for cultural and linguistic diversity. When assessing these students, a language/developmental history and caregiver input are essential.
Standardized Assessments
- Bilingual Administration: Administer assessments in the student’s primary native and secondary languages if available (e.g., CELF-Spanish or GFTA-Spanish). If a bilingual SLP is not available, an interpreter should be used.
- Modifications: Accommodations to standardized procedures may be necessary. Any non-standardized administration and the resulting lack of validity for standard scores must be noted in the evaluation report.
- Scoring: Standard scores should NOT be reported if a test has been translated. While translated tests provide helpful qualitative data, the numerical scores are not valid.
Criterion-Referenced and Dynamic Assessments
- Informal Assessment: These can be less-discriminatory resources for understanding a student's functional abilities. Reports should describe tasks, presentation methods, and the reasoning behind conclusions.
- Language Sampling: Samples in all used languages offer insight into functional morphology, syntax, phonology, and lexical systems. Clinicians should remember that skills across languages may not have a one-to-one correspondence.
Eligibility
Under Federal law (IDEA 2004), communication difficulties must not be due to cultural or linguistic differences. SLPs should consider the five characteristics of second language learning (Roseberry-McKibbins, 2002):
- Interference (Transfer): First language influences English use.
- Interlanguage: Rules change as the new language is learned.
- Silent Period: Listening to the new language with limited verbal output.
- Code-switching: Alternating between English and a native language.
- Language Loss: Decreased skills in the first language as English is acquired.
Service Delivery
Goals should reflect weaknesses in the dominant language, not weaknesses due to limited English proficiency. Teaching English as a second language is not the role of special education. Monolingual SLPs can support multilingual learners by using visual aids, collaborating with EL staff, and training paraprofessionals to provide language support.
Assessments for Multilingual Learners
- Alberta Language and Development Questionnaire (ALDeQ)©(External PDF, opens in new window)
A parent-reported measure of first language development designed for English language learners, regardless of specific language/cultural background.
- Family Socio-Cultural Interview(PDF, opens in new window)
Assessments by Language or Dialect
- Spanish: PLS-5 Spanish, CELF Preschool-2 Spanish, CELF-4 Spanish, BESA, Spanish SPELT-3, GFTA-3 Spanish.
- Arabic: The Arabic Language: Assessment of Function.
- African American Vernacular English: Diagnostic Evaluation of Language Variation (DELV).
Additional Resources
Low Incidence Populations
Overview
This section discusses the SLP's role in supporting students with low incidence disabilities, including those with primary eligibilities of Cognitive Impairment, Severe Multiple Impairment (SXI), Physical or Otherwise Health Impaired (POHI), Deaf and Hard of Hearing (DHH), Visual Impairment (VI), or Autism Spectrum Disorder (ASD). Many of these students present with Complex Communication Needs (CCN) that require collaborative support from both the SLP and the classroom teacher.
Evaluation
ASD Evaluation
- Multidisciplinary Team: Per MARSE, the team must include a school psychologist or psychiatrist, a school social worker, and an SLP. Other professionals (OT, TC) may be included as needed.
- Observational Data: Evaluations should rely heavily on observations across academic and non-academic settings by all team members.
- MARSE Eligibility Observation Form for ASD(PDF, opens in new window)
SXI Evaluation
- Informal Assessment: Due to sensory and physical limitations, standardized tests may not be feasible. Evaluations should prioritize caregiver/teacher interviews, developmental history, and functional tools.
- Communication Matrix(External Website, opens in new window)
- Interactive LCPS Continuum of Language Expression(Google Sheets, opens in new window)
Service Delivery
Speech-language services should align with the complexity of the student's needs and developmental milestones. Direct services are prioritized for preschool and early elementary. For upper elementary and beyond, consultation and push-in models are prioritized, provided the student's needs can be effectively met within the center-based program supports.
The primary goal is to ensure the student becomes an autonomous communicator with functional skills for the school environment, including unstructured times like lunch and recess. Collaborative pragmatic goals involving the SLP, Social Worker, and OT are strongly encouraged to promote generalization of skills.
Exit Considerations
If a student’s speech-language needs are being effectively addressed through specialized instruction provided by the special education teacher or categorical program, the SLP may not be required to continue services. This shift must be supported by quantified data within the PLAAFP demonstrating that specialized instruction from the SLP is no longer warranted for FAPE.
Additional Resources
- Evaluation Team Observation Form & Probe Questions(PDF, opens in new window)
- The Education-Based Evaluations for Autism Spectrum Disorder (MDE)(PDF, opens in new window)
- MARSE Eligibility Observation Form for ASD(PDF, opens in new window)
- Communication Matrix Assessment Tool(External Website, opens in new window)
- The Interactive LCPS Continuum of Language Expression(Google Sheets, opens in new window)
Augmentative and Alternative Communication (AAC)
Overview
Communication is the essence of human life and a fundamental right. Augmentative and Alternative Communication (AAC) supplements or compensates for impairments in speech-language production or comprehension. It is a multimodal approach that incorporates an individual’s full range of abilities, including existing speech, vocalizations, gestures, manual signs, and aided communication devices. AAC supports fall under the category of Assistive Technology (AT), which must be considered for every student receiving special education services under IDEA/MARSE.
Evaluation & Eligibility
There are no prerequisites to begin using AAC. No specific cognitive level, physical ability, or minimum age is required. AAC should be considered for students who are non-speaking, as well as those with speech that is unintelligible to unfamiliar listeners. Research confirms that AAC does not delay verbal speech; rather, it often supports language development.
The goal of AAC is autonomous communication: the ability to say whatever they want, whenever they want, to whomever they want. Assessment is a collaborative, ongoing process guided by the SETT Framework (Student, Environment, Tasks, and Tools).
- Universal Core Vocabulary Board(PDF, opens in new window)
- SETT Framework Template(Google Doc, opens in new window)
- SETT Framework Resources (Joy Zabala, Ed.D.)(External Website, opens in new window)
Service Delivery
AAC therapy is language therapy. Implementation should occur during engaging, natural daily activities. A critical component of success is Aided Language Stimulation (Modeling), where communication partners point to symbols on the AAC system while speaking to support the student's comprehension and expressive growth.
Consultative services are often necessary to engineer the environment, program devices, and train staff and families to ensure the student has communication access across all settings.
Exit Considerations
Dismissal must be determined on a case-by-case basis. Before considering dismissal, the team should ensure the student can participate fully in interactions and has achieved the fundamental protections outlined in the Communication Bill of Rights. A transition plan for device maintenance and partner training must be in place prior to exiting services.
Additional Resources
Early Childhood Speech & Language Overview
Overview
 Early intervention is a system of services designed to support infants, toddlers, and preschoolers with developmental delays or disabilities. These services focus on the first three years of life, targeting physical, cognitive, communication, social/emotional, and self-help skills. The Individuals with Disabilities Education Act (IDEA) mandates services for infants and toddlers under Part C and for children ages 3-5 under Part B.
Early intervention is a system of services designed to support infants, toddlers, and preschoolers with developmental delays or disabilities. These services focus on the first three years of life, targeting physical, cognitive, communication, social/emotional, and self-help skills. The Individuals with Disabilities Education Act (IDEA) mandates services for infants and toddlers under Part C and for children ages 3-5 under Part B.
The primary goal is to enable young children to be successful participants in their homes, childcare, preschool, and the community. In Wayne County, most referrals are due to speech concerns, making the SLP a critical team member who may serve as the Primary Service Provider (PSP) or provide expert support to the team.
Definitions
- Part C (Early On): Services for infants and toddlers from birth to age 3.
- Part B (Early Childhood Special Education): Services for children ages 3 to 5 years.
- Primary Service Provider (PSP): A specific team member who serves as the main point of contact and connection between the family and the multidisciplinary team.
Evaluation & Eligibility
Eligibility for Early On (Part C) is met when an infant or toddler exhibits a 20% delay in any developmental area or has a known established condition. Early Childhood Special Education (Part B) eligibility is determined when a child meets specific MARSE criteria following a formal evaluation.
Child Outcomes
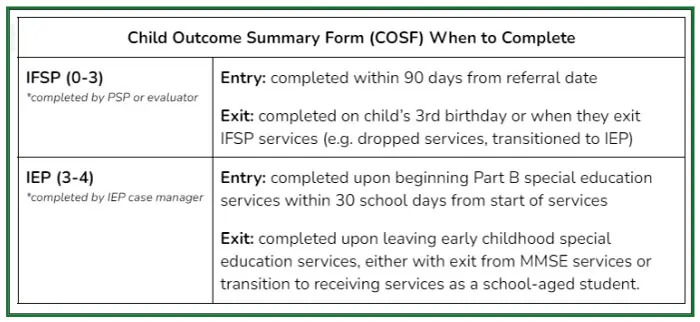 The Child Outcome Summary (COS) process synthesizes information on a child’s progress across multiple settings. Reporting is required at both entry and exit of services to measure progress and improve service delivery. The IFSP/IEP Team must use tools that assess all developmental domains (e.g., Brigance, Carolina Curriculum, MEISR).
The Child Outcome Summary (COS) process synthesizes information on a child’s progress across multiple settings. Reporting is required at both entry and exit of services to measure progress and improve service delivery. The IFSP/IEP Team must use tools that assess all developmental domains (e.g., Brigance, Carolina Curriculum, MEISR).
Service Delivery and Family Involvement
Early On services are typically provided within the child’s natural environment (home or community) and are offered year-round. Services for children ages 3-5 generally align with the school district’s calendar. Parents and guardians are essential partners in every stage of the process—from evaluation and planning to service delivery and transition. Family engagement is the most significant factor in achieving positive long-term outcomes for the child.
Early OnⓇ - Birth to 3 years old (IDEA PART C)
Overview
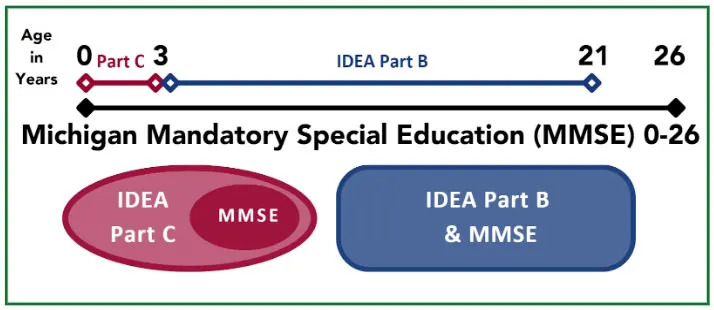
Early OnⓇ provides services to children from birth to 3 years of age (0-36 months) who are at risk for developmental delays and/or disabilities. While federal IDEA regulations cover special education services for children ages 3-21, Michigan Mandatory Special Education (MMSE) extends this range from birth to age 26. In Michigan, the Department of Education coordinates these services across school and non-school agencies. Once a referral is received and eligibility is confirmed, an Individualized Family Service Plan (IFSP) must be developed within 45 calendar days.
Evaluation
Best practice warrants a play-based evaluation conducted in the child's natural environment. Eligibility is determined through informed clinical opinion derived from multiple sources:
- Multidisciplinary Team: Assessment is completed by the caregiver and two evaluators from different disciplines (e.g., SLP, Teacher, OT, PT, Social Worker, or Psychologist).
- Adjusting for Prematurity: Required for every child born at 36 weeks gestation or earlier. This adjustment must continue until the child reaches a chronological age of 24 months.
- Information Gathering:
- Hearing and vision screenings.
- Medical documentation and health appraisals from the child's doctor.
- Routines-based assessments and informal observations.
- Observation of parent-child interaction and developmental history.
- Evaluation of all developmental domains: adaptive, cognition, communication, motor, and social-emotional.
Eligibility
Eligibility focuses on the functional impact of a delay on a child's participation in daily routines, play, and interactions. The suspected disability must not be due to limited English proficiency. After a child reaches two years of age (chronologically), adjustments for prematurity are discontinued.
Early On Criteria:
- Established Conditions: For children with a pre-existing condition on the state-approved list, a formal evaluation tool is not required to establish eligibility, though information gathering must continue.
Early On Established Conditions List(PDF, opens in new window) - Developmental Delay:
- Children under 2 months old (adjusted age): Any documented delay.
- Children 2 months to 36 months old: A delay of 20% or 1 standard deviation below the mean in one or more developmental domains.
Informed Clinical Opinion: This makes use of qualitative and quantitative information to assist in forming a determination regarding difficult-to-measure aspects of developmental status. It may be used to recommend eligibility but cannot be used to negate the results of evaluation instruments used to establish eligibility.
Additional Factors to Consider
The following areas are predictive of later language outcomes and should be scrutinized during the evaluation process:
- Communication Profile: Functions, means, and frequency of communication; rate of vocabulary growth (especially verbs); and early sound development.
- Developmental Markers: Imitative skills, play skills, emergent literacy, and oral motor/feeding systems.
- Social-Environmental Factors: Parent-child interactions, level of caregiver concern, and environmental stressors.
Resources
Preschool Special Education: 3 to 5 years (Part B)
Overview
IDEA Part B qualifies children and youth ages 3 through 21 to receive special education and related services, ensuring a Free Appropriate Public Education (FAPE) in the Least Restrictive Environment (LRE). While preschool is not mandated in Michigan, children ages 3-5 have full access to these services. A referral can be made by anyone, but the legal caregiver must consent to the evaluation. Intake staff should gather developmental concerns through a caregiver interview during the scheduling process.
Part B services may begin when a child turns 2 years and 6 months old:
- Transition from Part C: If a child has an Individualized Family Service Plan (IFSP), a transition plan and conference must occur between the ages of 2 years 3 months and 2 years 9 months to support the move to an IEP.
- Initial Referral: If a child is identified after age 3, an IEP must be completed within 30 school days from the start of the referral.
Evaluation
Best practice warrants a play-based evaluation conducted in a natural environment with parent/caregiver participation. Evaluators should use an all-domain assessment tool (such as the Battelle Screener) alongside observations and interviews to determine eligibility and report required Child Outcome Summary (COS) data.
- Child Find Procedural Guide(PDF, opens in new window)
- Child Outcome Summary (COS) Data Resources(External Website, opens in new window)
Eligibility
Eligibility is determined by a team, including the parent, based on a comprehensive analysis of data rather than a single assessment. The evaluation must be non-discriminatory and cover all areas related to the suspected disability, including health, vision, hearing, social-emotional status, general intelligence, communicative status, and motor abilities.
There must be documented evidence of adverse impact on the child’s participation in age-appropriate activities, such as daily routines, play, and social interactions. The suspected disability cannot be due to limited English proficiency.
Transition & Exit Considerations
Transition planning requires active participation from the Primary Service Provider (PSP), families, and receiving preschool or school staff to ensure continuity of services. Before exiting an Early Childhood program, a comprehensive evaluation must assess whether the child has achieved their goals and if further speech-language services are necessary.
To support a successful move to a new program or school district, all relevant records—including progress reports, assessments, and the current IEP—must be transferred to ensure the new team understands the child's progress and required supports.
FAQ: Caseload / Workload Service Delivery
Service Delivery Models
| Direct | Consult |
|---|---|
| Provider works directly with the student. | Provider observes, informally assesses, or works with the student. |
| Work with the student is related directly to the goals and objectives (may be collaborative with another provider). | Provider consults with the teacher and/or parent/guardian; activities are related to goals and objectives that the team is working on. |
| Progress reports are completed by the related service provider. | Progress reports are completed collaboratively by both the teacher and the related service provider. |
| Provider documents service provisions. | Provider documents service provision and consultation activities. |
| The student is counted on the provider’s caseload. | The student is counted on the provider’s caseload. |
Frequently Asked Questions
1. How do the roles and responsibilities of the various levels of service compare? Please refer to the service delivery table above for a side-by-side comparison of direct and consultative roles.
2. How do I document direct/consultative services in the IEP? Direct and/or consultative services should be documented separately and include the total time and frequency that each service will be provided.
3. Do I need to complete a REED if adding/dismissing speech-language as a related service? If the student has met their IEP goals and objectives and it is determined that there are no other identified speech-language areas of need, then speech-language as a related service can be dismissed without completing a REED. Instead, you may use progress monitoring data to provide information needed in the PLAAFP to dismiss the service. However, if you are collecting data through a formal process (assessment, observation, etc.) to determine the need for related services, then a REED is required for determining a need for service or to exit the service and for parent/guardian notice. IDEA states that if the IEP Team determines no additional data is needed, the district must notify the parent/guardian of that reason.
4. What might a caseload look like that abides by MARSE rules? Completing ASHA’s Workload Calculator(opens in new window) is the first step to determine an appropriate caseload size. This should consider severity and multiplicity of disabilities, diagnostics, report writing, consulting, meetings, and travel between buildings.
5. Do initial evaluations count toward caseloads? Yes, MARSE specifically states that evaluations "shall be counted as part of the caseload." Any student being evaluated counts toward the caseload cap. One evaluation is equivalent to one caseload student. This applies to initial evaluations, re-evaluations, and Child Find assessments.
6. What should a caseload look like for a SLP providing birth-3 services? Considerations include the PSP/transdisciplinary approach with parent coaching, frequency/length of visits (45-60 minutes), parent education, travel time, Part C to Part B transitions, weekly evaluations, and bi-annual reviews of IFSPs.
7. How should an IEP Team determine a Designated Case Manager? The team should consider the nature of the disability, service time, and staffing availability. While the staff member with the most frequent contact often assumes this role, the team should prioritize the provider most appropriate to ensure the behavioral or physical needs of the IEP are implemented correctly.
8. How should monitoring be counted? Monitoring should be used cautiously. It should only be utilized if it supports a measurable outcome for the student in the Least Restrictive Environment (LRE). In these instances, a workload analysis approach is recommended.
FAQ: Evaluation / Eligibility Overview
Evaluation and Eligibility FAQ
1. If a SLP participates in a multidisciplinary evaluation for other eligibility areas (e.g., CI, ASD, SLD), must SLI be considered as an additional area? If the SLP is a team member but SLI is not the primary concern, the Eligibility Report does not have to reflect that SLI was considered. however, in the REED document, you must check the box for "Appropriate programs or services in special education" within the "Purpose" section.
2. How are outside evaluations incorporated into a school evaluation? Information from outside reports, including standardized data, should be reviewed as part of the evaluation process. This data should be included in the REED and/or Eligibility Recommendation. If provided outside of an evaluation cycle, the IEP Team should reflect the information within the IEP or through Prior Written Notice by initiating a REED if needed.
3. Does absenteeism or lack of curriculum exposure disqualify a student for eligibility? No. When considering speech and language concerns, these factors do not discount a student for eligibility. The evaluation team must look at the whole student rather than a specific period of time.
4. Should age or grade equivalent scores be used in making eligibility decisions? No. Equivalents do not account for normal variation around the test mean and are not on an equal interval scale. They do not relate to curriculum content and are highly subject to misinterpretation. They should not be used to determine whether a student has a significant deficit.
5. Can you modify standardized test procedures? Modifying procedures invalidates the use of test norms but may provide helpful qualitative information. If administration is invalid for any reason, scores should not be subjected to usual interpretations, and the reasons for invalidation must be clearly stated in all presentations of results.
6. Can one-word vocabulary tests be used to qualify students for services? These should be used with extreme caution. Studies have found that single-word vocabulary tests often have poor psychometric properties and are not representative of linguistic competence in functional life activities.
7. Who can sign as a parent/guardian on a REED? Per MARSE, a "Parent" includes: (i) Biological or adoptive parent; (ii) A foster parent (unless prohibited by law); (iii) A legal guardian; (iv) An individual acting in the place of a parent (grandparent, stepparent, etc.) with whom the child lives; or (v) An appointed surrogate parent if the child is a ward of the state.
8. What if a parent/guardian refuses to sign consent for an initial evaluation? The district may not proceed with the evaluation. If the district disagrees with the refusal, the team should contact the Director of Special Education to discuss potential next steps and options.
9. What if a parent or student (age of majority) requests to discontinue services while still eligible? The parent or student must sign a Revocation and Notice of Cessation to discontinue services. You should notify your Special Education Administrator and follow local district procedures for this process.
FAQ: Speech Sound Disorders
Articulation and Speech Sound FAQ
1. What do you do when a student is not making progress? Various methods and strategies should be employed and documented prior to any service level reduction. Decisions to remove services should consider the student’s response to intervention (RtI) and attempts to redesign the service delivery. If a student has plateaued despite these attempts, the team may discuss a lack of educational benefit with district administrators. Refer to MSHA (2006) SLRS-4 for more information.
2. Do you consider developmental norms when treating lateralization? Lateralization of /s, z, sh, ch, j/ does not typically improve spontaneously with age and is not considered developmental. Eligibility should be determined through further investigation of stimulability, prognosis, response to early intervening, and adverse educational effect.
3. What about students with single sound errors? Adverse educational effect should be considered seriously for single sound errors, as these students often face challenges with social relationships, literacy, and vocational outcomes. Early intervention (direct or indirect) can be highly effective. It is imperative to support educational needs regardless of the number of sounds in error.
4. Does dentition or tongue thrust impact speech sound production? Yes. Dentition and tongue movements should be evaluated with an oral peripheral exam. To be eligible for articulation services, students with these differences must demonstrate a speech disorder that adversely affects school performance. Oral Peripheral Mechanism Examination Form(PDF, opens in new window)
5. When should you consider using an augmentative/alternative communication (AAC) system? Strong consideration should be given to AAC when a student is making slow progress in treatment and there is a significant impact on academic or social communication due to poor speech intelligibility. Refer to the Augmentative and Alternative Communication section above.
6. Do students with a history of cleft lip/palate respond to speech therapy? Treatment response depends on whether deviations are obligatory (structural/anatomical) or learned:
- Obligatory deviations: Related to true VPD or fistulas; these are not responsive to speech therapy and usually require surgical or physical management.
- Learned errors: Compensatory errors and phoneme-specific nasal air emission should be responsive to speech therapy.
7. Do you need two standardized scores to qualify a student for an articulation impairment? No. While you must use at least two different evaluation tools, they do not both need to be standardized tests. You may use a combination of a standardized score, observations, caregiver/teacher input, or speech sample analysis (e.g., Intelligibility or PCC).
8. If a student has a phonological processing disorder, is it Articulation or Language? Per ASHA’s definition of Speech Sound Disorders as an umbrella term, Wayne RESA recommends using the sub-area of Articulation for all impairments in speech sound disorders where this is the primary impairment.
FAQ: Language
Language and Dynamic Assessment FAQ
1. How do you distinguish a language impairment from a language difference? A student must present with a language disorder in both languages to qualify as having a language impairment. To differentiate, teams should ask:
- Does the student present with average language skills in their home language?
- Is the student learning English at a similar rate to comparable peers?
"No" answers to these questions may indicate an impairment, while "Yes" answers typically indicate the natural process of English language learning.
2. How do you distinguish a language impairment from an attention difficulty? One way to differentiate is to observe if strategies like repetition and active listening significantly improve comprehension. For example, if a student fails to follow a direction but succeeds once they are prompted to use active listening (eyes on speaker, calm body) and the direction is repeated, the issue may be attention-based. If they still cannot respond correctly after these supports, it may indicate a receptive language difficulty.
3. How do you distinguish a language impairment from a behavior difficulty? Investigate if the student is able to exhibit the skill at all or only under certain circumstances. If a student only responds to a direction when given an incentive, they likely understood the instruction but chose when to comply. If the student cannot perform the skill despite high motivation or incentives, it may indicate a lack of the underlying language skill rather than a behavioral choice.
4. How do you effectively evaluate pragmatic language? Evaluation must address three major areas: communicative intent, nonverbal rules, and verbal rules of conversation. SLPs should address both developmental expectations and functional efficiency. Assessment should rely on developmental checklists, parent/teacher reports, and direct observations across various school environments and social interactions.
5. What is meant by Dynamic Assessment? Dynamic assessment identifies a student's current skills and their potential for learning. Unlike static assessments (standardized tests) which measure previously learned knowledge, dynamic assessment uses a test-teach-retest method. This is especially helpful for culturally and linguistically diverse students: those who make significant changes during short-term teaching likely have a language difference, while those who do not may have an impairment.
6. What is a Social Communication Disorder? According to ASHA, children with language disorders may also present with persistent difficulties using verbal and nonverbal language for social purposes.
ASHA Practice Portal: Social Communication Disorder(External Website, opens in new window)
FAQ: Fluency
Fluency and Stuttering FAQ
1. How do you differentiate between typical speech disfluencies and stuttering? Stuttering typically begins between ages 2 and 6. Typical (non-stuttered) disfluencies include hesitations, interjections (e.g., "um," "like"), whole-word repetitions, and phrase revisions. Stuttering-like disfluencies include part-word repetitions, sound prolongations, and blocks, often accompanied by physical tension or extra effort. Differential diagnosis is critical when a student shows a high frequency of typical disfluencies to distinguish between stuttering, avoidance, and language disorders.
2. How do you distinguish cluttering from stuttering? Cluttering is characterized by a rapid or irregular speech rate, excessive coarticulation (collapsing syllables), and disfluencies that are usually "non-stuttering" types (revisions and fillers). Unlike students who stutter, those who clutter are often less self-aware of their speech. Key diagnostic features of cluttering include poorly organized thinking and short attention spans. A thorough language evaluation, including written expression, is necessary if cluttering is suspected.
3. What are the Risk Factors associated with stuttering?
| Risk Factor | Elevated Risk Indicators |
|---|---|
| Gender/Sex | Male (affects males 3-4x more than females). |
| Family History | Family history of persistent stuttering. |
| Total Time Since Onset | Duration of 6-12 months or more with no improvement. |
| Pattern of Stuttering | Presence of prolongations, blocks, and secondary behaviors. |
| Awareness | High levels of student awareness or frustration regarding disfluencies. |
| Co-occurring Impairments | Presence of other phonological or language impairments. |
| Sensitivity | Emotional sensitivity or reactive temperament in stressful situations. |
4. What are the exit considerations and the role of a 504 plan? When a student no longer requires specialized instruction but still has a disability that limits major life activities, a 504 plan should be considered. Accommodations may include:
- Using audio/video recordings for oral presentations.
- Increasing time for oral reading or presentations.
- Providing alternative assignments to oral reading.
- Altering group size or audience for presentations.
- Allowing the student to ask questions to the teacher in private.
5. What about atypical disfluencies and traditional intervention? Atypical disfluency involves broken sounds or repetitions at the ends of words (e.g., final sound prolongations). These are often not responsive to traditional fluency therapy. The SLP must determine how coexisting disorders (e.g., Autism, ADHD, or Down Syndrome) influence speech and adjust treatment to focus on overall communication management.
6. Are there special factors for bilingual students who stutter? Yes. Bilingual students who stutter typically do so in both languages. They may produce more "mazes" (word tangles) than monolingual peers, which can be misdiagnosed as stuttering. Diagnosis must be based on the presence of audible/inaudible prolongations, excess tension, and parent concern across both languages.
FAQ: Linguistic Diversity and Multilingual Learners
Multilingual Learners and Linguistic Diversity FAQ
1. How does the dominant language influence English learning in terms of disability? IEP goals must reflect areas of weakness present in the dominant language, not weaknesses resulting from limited English proficiency. Special education is not intended to teach English as a second language.
Language Influence Chart(Google Doc, opens in new window)
2. How does Language 1 (L1) influence speech sounds in Language 2 (L2)? Assessment of articulation, fluency, or voice must rule out limited English proficiency as a factor. Assessments should occur in the student’s native language to determine if needs are present in L1 or are culturally influenced.
ASHA: Phonemic Inventories Across Languages(External Website, opens in new window)
3. When should I evaluate, considering the "silent period" of language acquisition? There is no standard "wait time." Per Child Find, an evaluation must be conducted whenever a disability is suspected. However, teams should carefully consider language differences, acculturation, and the efficacy of the EL program prior to formal testing.
4. How long should I wait to evaluate students who are new to the country or newly adopted? If there is a known established condition (e.g., Down Syndrome, Cleft Palate, Cerebral Palsy), the team must proceed immediately. In other cases, monitor performance relative to peers and response to language support. Evaluation should not be delayed solely due to English proficiency status, but proficiency must be ruled out as the primary cause of difficulty.
5. Are there culturally sensitive parent input forms available?Multilingual Family Input: Socio-Cultural Interview(Google Doc, opens in new window)
6. Do I need to use the exact same test in both languages? No. Tests rarely have a 1:1 correspondence across languages. Translating a standardized English test (e.g., CELF-5) with an interpreter is discouraged as it invalidates norms. Use assessments designed specifically for the native language when available, and always consider cultural background in the results.
7. How do I effectively work with an interpreter or EL staff? The SLP remains responsible for the session plan and material selection.
- Before Assessment: Review roles, key phrases, and procedures. Remind the interpreter not to alter, omit, or add to the student's communication.
- Cultural Context: Ask the interpreter about specific words that may not be translatable or cultural considerations for the testing event.
8. Can students with an IEP also receive EL support? Yes. A student qualifying for EL services may receive both special education and EL support if the IEP Team determines both are necessary for the student to access the general education curriculum. If EL support is needed, ensure the "Special Factors" page of the IEP reflects this.
9. What are the federal requirements for EL evaluations? School districts must consider English proficiency when determining which assessments to use. The IEP team must include participants with knowledge of the child’s language needs.
Joint DCL: English Learner Students and Limited English Proficient Parents(PDF, opens in new window)
FAQ Low Incidence Populations
Placement and Discharge FAQ
1. When might a student no longer require direct or consult speech-language services due to their current placement?
- Embedded Programming: If language needs and interventions are already embedded within a student's current self-contained classroom curriculum, the student may not require separate SLP services. The team must ensure the IEP goals align with the classroom curriculum and that functional language needs are met within that setting.
- Mutual Decision for Discharge:Discharge is ideal when the student, family, and SLP agree that:
- The communication disorder has been remediated or compensatory strategies are established.
- The individual or family chooses to opt-out, relocates, or seeks a different provider.
- Multiple treatment modifications have been attempted, but measurable benefits are no longer observed.
2. Is it appropriate to discharge a student from a speech caseload due to a "lack of progress"? A perceived lack of progress often indicates that the current intervention, methods, or data collection are a poor fit for the student. Before considering discharge, teams should:
- Examine if the intervention is optimal for the individual and their educators.
- Provide direct support and training for family members and stakeholders to clarify the role of families as agents of change.
- Consider competency-based training (e.g., Schepis and Reid, 2003) to promote the application of treatment across all settings.
3. How should we support students with speech-language needs within self-contained classrooms? If specialized instruction within the self-contained program already meets the student's speech-language needs, SLP services are not required. However, if the environment or student needs change, the team must consider reestablishing services. The PLAAFP must include quantified data points demonstrating how these needs are being met through the alternate program/service.
4. How are communication needs addressed for a student with ASD who does not currently receive speech services? A student may meet ASD eligibility criteria regarding qualitative impairments in communication without requiring direct SLP services if those needs are met by the current placement or other providers. A thorough evaluation using both formal and informal measures is necessary to differentiate between eligibility (meeting ASD criteria) and service need (requiring specialized SLP instruction).
FAQ: Augmentative and Alternative Communication
AAC (Augmentative and Alternative Communication) FAQ
1. Is a REED required to consider AAC options for a student? A REED is not required to consider AAC options unless formal standardized testing (such as specific receptive/expressive language batteries) is necessary for the decision-making process. In those cases, a REED must be completed first.
2. When should AAC be considered for a student? AAC should be considered whenever a student's speech output is inadequate to communicate their wants and needs. Factors to consider include frustration levels (student and partner), access to curriculum, ability to demonstrate knowledge, and independence in daily activities.
3. Should AAC be used as a supplemental strategy to traditional speech intervention? Yes. If a student is making slow progress and speech intelligibility significantly impacts their social or academic life, AAC should be used to increase overall communication. Research shows that early AAC intervention can actually support the development of verbal expression.
4. What if the SLP doesn't feel qualified to support AAC? Resources are available through the Wayne Assistive Technology Team (WATT) and district AT coaches. SLPs should seek professional development and guidance to ensure students have access to robust communication therapy.
5. Are there AAC equipment resources available to trial?
- Wayne Assistive Technology Team (WATT) Lending Library(Internal Link)
- Alt+Shift Lending Library(External Website, opens in new window)
6. Where should a recommended AAC system be documented in the IEP? If a student requires any tool to communicate (including light-tech boards), the need must be identified in the PLAAFP and included in Supplementary Aids and Services (SAS). It may also be reflected in transition plans or assessments.
7. Can you use specific brand names (e.g., iPad, TD Snap) in the IEP? No. Equipment should be described in general, feature-based terms. For example, use "access to a dynamic, robust, picture-based communication support system" rather than "iPad with TD Snap." Focus on the unique features necessary to support the student.
8. Are measurable goals needed if AAC is listed in Supplementary Aids? Yes. Communication goals should be developed to support AAC skill development.
Dynamic AAC Goals Grid-2 (DAGG-2)(PDF, opens in new window)
9. How do we document AAC if we are just starting to explore or trial systems? If needs are being explored, indicate in the Anticipated Needs section that a SETT Framework review is necessary. Once a specific need is determined but a trial is ongoing, you may list "SETT Framework Review to determine specific AT/AAC needs" in the SAS table.
10. Who is responsible for providing AAC equipment? Under IDEA, the school system is responsible for providing required AT/AAC items and the services needed to support them. Families may choose to pursue private funding for a personal system, but the district must provide what is necessary for the IEP.
11. What is a funding report? A funding report is a request to health insurance to cover an AAC system as a "medical necessity." Only an SLP can conduct this assessment and write the report. In Wayne County, WATT provides devices for students with moderate to severe disabilities; otherwise, the local district is responsible.
FAQ: Speech Sound Disorders
Articulation and Speech Sound FAQ
1. What do you do when a student is not making progress? Various methods and strategies should be employed and documented prior to any service level reduction. Decisions to remove services should consider the student’s response to intervention (RtI) and attempts to redesign the service delivery. If a student has plateaued despite these attempts, the team may discuss a lack of educational benefit with district administrators. Refer to MSHA (2006) SLRS-4 for more information.
2. Do you consider developmental norms when treating lateralization? Lateralization of /s, z, sh, ch, j/ does not typically improve spontaneously with age and is not considered developmental. Eligibility should be determined through further investigation of stimulability, prognosis, response to early intervening, and adverse educational effect.
3. What about students with single sound errors? Adverse educational effect should be considered seriously for single sound errors, as these students often face challenges with social relationships, literacy, and vocational outcomes. Early intervention (direct or indirect) can be highly effective. It is imperative to support educational needs regardless of the number of sounds in error.
4. Does dentition or tongue thrust impact speech sound production? Yes. Dentition and tongue movements should be evaluated with an oral peripheral exam. To be eligible for articulation services, students with these differences must demonstrate a speech disorder that adversely affects school performance.
Oral Peripheral Mechanism Examination(PDF, opens in new window)
5. When should you consider using an augmentative/alternative communication (AAC) system? Strong consideration should be given to AAC when a student is making slow progress in treatment and there is a significant impact on academic or social communication due to poor speech intelligibility. Refer to the Augmentative and Alternative Communication section of these guidelines.
6. Do students with a history of cleft lip/palate respond to speech therapy? Treatment response depends on whether deviations are obligatory (structural/anatomical) or learned:
- Obligatory deviations: Related to true VPD or fistulas; these are not responsive to speech therapy and usually require surgical or physical management.
- Learned errors: Compensatory errors and phoneme-specific nasal air emission should be responsive to speech therapy.
7. Do you need two standardized scores to qualify a student for an articulation impairment? No. While you must use multiple evaluation tools, you do not need to complete two standardized assessments to qualify for SLI in articulation. Best practice is to combine data from standardized scores, observations, caregiver/teacher input, or speech sample analysis (e.g., Intelligibility or PCC).
MARSE Guidelines (p. 35-36)(PDF, opens in new window)
8. If a student has a phonological processing disorder, is it Articulation or Language? Per ASHA’s updated definition of Speech Sound Disorders as an umbrella term for errors in articulation and phonology, Wayne RESA recommends using the sub-area of Articulation for all impairments in speech sound disorders where this is the primary impairment.
FAQ: Early Intervention - Early OnⓇ - Birth to 3 years old (IDEA PART C)
Early Childhood and Early On (Birth to 5) FAQ
1. When would you consider SLI eligibility vs. ECDD eligibility for birth to 5 evaluations? Early Childhood Developmental Delay (ECDD) is used only when a child’s primary delay cannot be attributed to another MARSE category. If a child meets ECDD criteria, they cannot meet any other eligibility rule.
- Functional Performance: For infants and toddlers, "functional performance" in daily routines and natural environments (home, childcare) is used as a substitute for "educational performance."
- Criteria: The delay must be equal to or greater than 50% (half) of the age equivalent in one or more developmental areas.
- Example: If a child has a 50% delay in both speech and cognition, ECDD may be appropriate because it is unclear if the delay is primarily a speech impairment or a more global cognitive deficit.
ECDD Guidance for Birth to Age Three(PDF, opens in new window)
2. When do you consider SLI vs. ASD eligibility for Part C (Birth-3)? Teams should not use a "wait and see" approach (e.g., using SLI or ECDD temporarily) if an infant or toddler meets the criteria for Autism Spectrum Disorder (ASD).
- If a comprehensive assessment shows the child meets ASD criteria, the team must provide that recommendation.
- Eligibility should always reflect the primary area of need as it relates to functional impact.
3. How are frequency and duration of home visits determined for an IFSP? Early intervention teams determine service levels based on the unique needs of the child and family. Factors include the caregiver's learning style, social/cultural factors, and the support needed to develop a successful caregiver-professional partnership. Services should be monitored and modified based on results.
4. Who is responsible for transition planning in early childhood? The Primary Service Provider (PSP) or IEP case manager facilitates communication with the parent and the next transition site (e.g., LEA representative). The district of residence is responsible for the initial IEP transition.
5. If a child is 2 years and 6 months old, do I complete an IFSP or an IEP? Per MARSE, children at 2.6 years may receive an IEP. However, families must be given the option to continue with an IFSP until the child turns 3. Consider factors like community preschool attendance, the time of year, and whether the family is ready for an educational versus a family service plan.
6. Can an SLP provide feeding or dysphagia therapy within an IFSP? Yes. SLPs can provide therapy for feeding, dysphagia, or oral motor dysfunction within an IFSP. Goals should remain child and family-driven, utilizing caregiver coaching for implementation.
7. How can someone make a referral to Early On? Anyone can make a referral; evaluations are provided at no cost in the family's home.
- Early On Michigan: 1-800-Early-On or miearlychildhood.org.
- Wayne County Referral Hotline: 734-334-1393.
FAQ: Special Interest Topics
Wayne RESA provides the following guidance on special interest topics. For further reading, see the Kent ISD Speech and Language Guidelines (pages 82-97)(Google Drive PDF, opens in new window).
Auditory Processing Disorders (APD/CAPD)
Could a student be eligible under Section 504 with a CAPD diagnosis? Yes. If the disability substantially limits a major life activity and requires accommodations to access the school environment, a student may be eligible for a 504 plan.
Deaf and Hard of Hearing (DHH)
1. Who is responsible for completing standardized language assessments? Primarily the SLP, though a certified DHH teacher or Teacher Consultant may also conduct these assessments. The team must consider the student's primary language modality (e.g., using an ASL interpreter if the evaluator is not proficient in ASL).
2. How do we determine if DHH or SLI is the most appropriate primary eligibility? The IEP team must determine if the impairment is a direct result of hearing loss and auditory access (DHH) or a specific communication disorder (SLI). MARSE distinguishes "Deafness" (auditory channel is impaired for processing linguistic info) from "Hard of Hearing" (auditory channel remains the primary means for developing language).
3. What factors are considered when exiting special education for a 504 plan? The team must evaluate adverse impact on academics and social-functional communication. A 504 plan may include:
- Strategic seating (away from HVAC or noise).
- Access to captions for instructional videos.
- Use of Remote Microphone Technology (FM systems).
Dysphagia (Feeding and Swallowing)
1. Does a school SLP need to address dysphagia? Yes, it falls within the SLP scope of practice. If a student demonstrates a need that impacts their school day, the SLP should be part of a school-based dysphagia team.
2. What is the procedure for a swallow study referral? The SLP advises the parent to consult their physician for a medical swallow study. The school SLP should obtain a release of information to coordinate with the medical SLP or doctor.
3. What is the SLP's role in dietary recommendations? Caloric and dietary types are set by a doctor or dietitian. The SLP ensures these are implemented at school and assists with food consistency, positioning, and feeding tools.
Selective Mutism (SM)
1. What if the student does not speak during the evaluation? Non-participation is itself diagnostic data. SLPs should use home audio/video recordings to observe the student's "best" communication in private settings to compare with school performance.
2. How does SM impact articulation and language? Articulation and receptive language are typically normal, but anxiety may cause the student's voice to sound "different." Expressive language may show subtle deficits simply due to a lack of practice in social domains.
Secondary Students (Middle and High School)
1. When is articulation therapy appropriate at the secondary level? It is considered if there is a documented adverse impact on transition/vocational goals, the student is highly motivated, and the team acknowledges the removal from general education curriculum time.
2. Can a SLP support concerns on the IEP transition page? Yes. If a student has pragmatic needs for job interviews or post-secondary life but doesn't require a related service, the SLP can consult on transition activities instead.
3. How is language supported in self-contained classrooms? If needs are met by the specialized program curriculum, direct SLP services may not be required. However, the SLP may provide "Support for School Personnel" to coach staff on maintaining communication fidelity within the room.